
Cardiopulmonary resuscitation. CPR. I remember sitting in
junior high school and high school health class, rolling my eyes for every “CPR
training session”. Secondary education spent entire months dedicated to
teaching CPR. Why? I saw no point in them because I thought I’d never end up in
a situation where I would need CPR. I thought everyone and everything was
invincible. Now, at the end of my 4th year in college, I can see how
important these procedures are. I have also seen a very inconvenient truth
about CPR. No matter how much we learn or how much class room time we spend on
CPR, its failure rate is definitely higher than its success rate.
The point of CPR is designed to preserve brain function. If
done properly it extends the chance for resuscitation through other means,
naturally or artificially. Idealistically, the factors of success with CPR
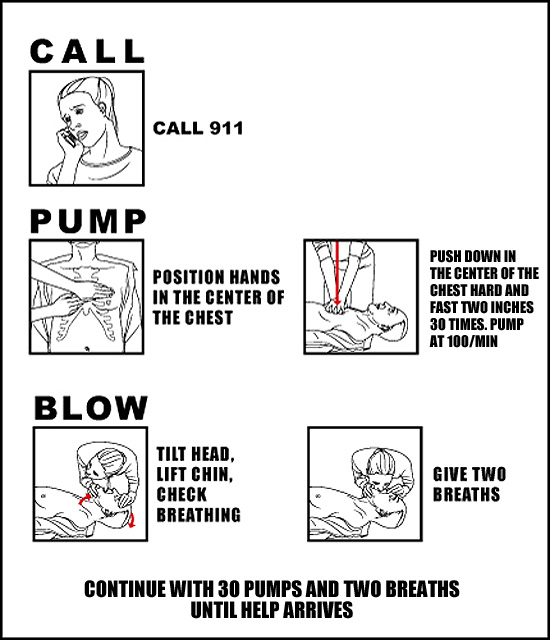
include:
- Compression depth of at least two inches
- Compression rate of at least 100 compressions per minute
- Allowing the chest wall to recoil fully between every compression
- Minimizing interruptions

The problem is that CPR is only designed to preserve brain functions
in the event of cardiac arrest. The probability of CPR actually restarting the
heart is statistically low, in contradictory to Hollywood’s glorification of
CPR. It can only limit tissue damage and minimize the amount of damage to the
patient’s brain. This problem stems from the manual nature of CPR. It’s similar
to putting a Band-Aid on a two inch laceration. You aren’t addressing the main
problem, instead you are attempting address the main problem indirectly by
attempting to solve a different issue. It will help, there is no doubt in that,
but overall it is a daunting task.
So you might be asking, who is this guy to bash on CPR? Well first, finish the paper. I am not bashing CPR but rather I am taking a very critical stance about CPR and two, I have been in 5 separate incidents that required CPR. One of the most notable situations is why I started exploring the realm of emergency medicine. It was a 55 mph head on collision that I ran across. In that situation, CPR was pointless but attempted none the less. I did what I was taught in high school, 30 compressions, 30 breaths. I did not allow the chest to fully decompress because I was in shock and not thinking, and my CPR technique was old. I really can’t help but think “what if” questions, such as, what if I was more up to date and aware about the “advancements” in CPR techniques. The advancements in CPR techniques include the movement towards soley using compression rather than balancing compression and artificial resuscitation (rescue breathing).
The second situation I was in that included CPR was the most
recent. I noticed a huge change in my mentality towards medical situations.
When I came upon that accident with Sean while driving up to a Spokane Airsoft
operation, we ran across the aftermath of a drowsy truck driver. I was calmer
and more educated, which led to initial success in quasi-securing the patient
without having any of the proper “tools” to C-Spine. I don’t even think Sean knows this (since he
was actively rerouting traffic for first responders) but we had to do a very
awkwardly positioned CPR. I will note
that we had no other choice and that we did our best to give the patient proper
spine support. We had no choice. I was in the proper position to do
compressions so I did so (while my temporary and BLS qualified partner
continuously checked C-Spine and her support).
It directly led to success. She began breathing roughly and her pulse
became more prominent (although still week). Although it led to initial
success, after paramedics and firemen showed up, she died. I did attempt CPR
again but to no avail. The blue palm was ominous.

CPR isn’t a nuclear option. Nukes work and they work well.
Think of CPR as a last resort. I will be blunt; I think CPR is futile but
necessary. If you need to do CPR, you have a more critical issue at hand.
However, as discouraging as I am, advancement in medical technologies and
practices have increased our ability to sustain and even improve brain functions
during a medical emergency. It’s not only critical for people to know these
potentially life-saving procedures but I feel that it should be a requirement.
As negative as I was earlier, I hold the view that if we can spend 50 minutes
of our time learning simple techniques can one day save a life, and then it’s
worth it. On top of that, public automated electrical defibulators (AED’s) are becoming more prominent and the
technology integrated in these AED’s are simple enough to use that I have seen
10 year old children successfully apply AED’s to dummies.
You may be confused by my point so I will sum everything all together. CPR’s job is to preserve brain functions and is highly unlikely to restart the heart; however CPR is highly glorified. It is not the save all technique. In fact, statistically, it is questionable at best. However, CPR is a necessary failure. CPR can and will continue to save lives. Even with increased availability in AED’s, we need to make sure that we aren’t technologically reliant. We need to take time out in our day to learn life saving techniques, not only CPR, in order to make sure when the time comes, if ever, that we are prepared. Don’t consider my failure stories as a discouragement to learning CPR; view them as a lesson to be learned from. CPR can potentially be a life-saving technique and it may grant your patient one last chance to say good bye. CPR is a successful failure.
You may be confused by my point so I will sum everything all together. CPR’s job is to preserve brain functions and is highly unlikely to restart the heart; however CPR is highly glorified. It is not the save all technique. In fact, statistically, it is questionable at best. However, CPR is a necessary failure. CPR can and will continue to save lives. Even with increased availability in AED’s, we need to make sure that we aren’t technologically reliant. We need to take time out in our day to learn life saving techniques, not only CPR, in order to make sure when the time comes, if ever, that we are prepared. Don’t consider my failure stories as a discouragement to learning CPR; view them as a lesson to be learned from. CPR can potentially be a life-saving technique and it may grant your patient one last chance to say good bye. CPR is a successful failure.
No comments:
Post a Comment